Should We Fall Out of Love with Robot Surgery?
The FDA is investigating whether doctors aren’t getting enough training before they start using machines to do surgery. Is the “wow” factor to blame?
/https://tf-cmsv2-smithsonianmag-media.s3.amazonaws.com/accounts/headshot/randy-rieland-240.png)
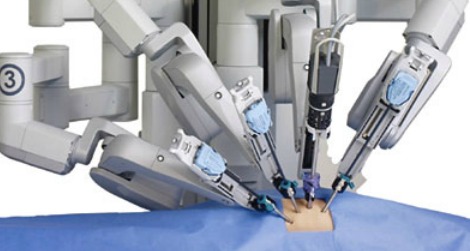

A da Vinci robot zeroes in. Photo courtesy of Intuitive Surgical
Last fall, shoppers outside a Macy’s store in Boston were given a chance to test drive a robot. They were invited, compliments of Brigham and Women’s Hospital, to sit at a console and move the machine’s arm the same way surgeons would in an operating room.
And why not? What says cutting-edge medicine more than robotic surgery? Who wouldn’t be impressed with a hospital where robot arms, with all their precision, replace surgeons’ hands?
The surgeons, of course, control the robots on computers where everything is magnified in 3D, but the actual cutting is done by machines. And that means smaller incisions, fewer complications and faster recoveries.
Usually.
But earlier this year, the Food and Drug Administration (FDA) began surveying doctors who use the operating room robots known as the da Vinci Surgical System. The investigation was sparked by a jump in incidents involving da Vinci robots, up to 500 in 2012.
The California company that makes the da Vinci, Intuitive Surgical, says the spike has to do with a change in how incidents are reported, as opposed to problems with its robots. It’s also true that robot surgery is being done a lot more frequently–almost 370,000 procedures were done in the U.S. last year, which is three and a half times as many as in 2008.
And the procedures are getting more complicated. At first, the robots were used primarily for prostate surgeries, then for hysterectomies. Now they’re removing gall bladders, repairing heart valves, shrinking stomachs during weight loss surgery, even handling organ transplants.
Unkind cuts
Not surprisingly, FDA survey has stirred up a swirl of questions about machine medicine. Have hospitals, in their need to justify the expense of a $1.5 million robot, ratcheted up their use unnecessarily? Has Intuitive Surgical placed enough emphasis on doctors getting supervised training on the machines? And how much training is enough?
It’s not an uncommon scenario for technological innovation. A new product gets marketed aggressively to companies–in this case hospitals–and they respond enthusiastically, at least in part because they don’t want to miss out on the next big thing.
But is newer always better? A study published recently in The Journal of the American Medical Association, compared outcomes in 264,758 women who had either laparoscopic or robotically assisted hysterectomies at 441 different hospitals between 2007 and 2010. Neither method is invasive.
But the researchers found no overall difference in complication rates between the two methods, and no difference in the rates of blood transfusion. The only big difference between the two is the cost–the robotic surgery costs one-third more than laparoscopic surgery.
Then there’s the matter of loosening training standards. When the FDA allowed the da Vinci system to be sold back in 2000, it was under a process called “premarket notification.” By claiming that new devices are similar to others already on the market, manufacturers can be exempted from rigorous trials and tough requirements. In this case, Intuitive Surgical was not formally required to offer training programs for surgeons.
The company did tell the FDA that it planned to require a 70-item exam and a three-day training session for doctors. But, as a recent New York Times article noted, Intuitive changed its policy just two years later. Instead it required surgeons to pass a 10-question online quiz and spend only a day in hands-on training.
So ultimately it’s up to the hospitals to set training standards. But in their rush to embrace the future, they can be tempted to avoid being too demanding. In one 2008 case that has resulted in a lawsuit against Intuitive, a patient suffered serious complications, including impotence and incontinence, while having his prostate gland removed. The surgeon, it turned out, had never done robotic surgery without supervision before.
A researcher at Johns Hopkins Hospital, Dr. Martin Makary, who has previously criticized hospitals for overhyping robotic surgery on their websites, has another study coming out soon that suggests that the problems involving da Vinci robots are underreported. “The rapid adoption of robotic surgery,” he contends, “has been done, by and large, without the proper evaluation.”
Dr. David Samadi, Chief of Robotics and Minimally Invasive Surgery at the Mount Sinai School of Medicine in New York, has a different way of looking at robotic surgery: “A good driver in a Lamborghini is going to win NASCAR. But someone’s who not a a good driver in a Lamborghini…he’s going to flip the car and maybe kill himself.”
Robots rising
Here are some other ways robots are being used in hospitals:
- Down go the mean old germs: Doctors at Johns Hopkins Hospital in Baltimore have turned to robots to take on the superbugs that have become such a threat of spreading dangerous infections among patients. After a hospital room is sealed, the robots spend the next half hour spraying a mist of hydrogen peroxide over every surface. Other hospitals are taking a a different approach in dealing with nasty bacteria–they’re using robots that zap germs with beams of ultraviolet light.
- And you’ll be able to see your face in the scalpel: GE is developing a robot that will keep the tools of the operating room sterile and organized. Instead of relying on humans doing this by hand–clearly not the most efficient process–the robot, by recognizing unique coding on each piece of equipment, will be able to sort scalpels from clamps from scissors, sterilize them and then deliver everything to the operating room.
- Bedside manner, without the bedside part: Earlier this year the FDA approved a medical robot called RP-VITA, which was developed by iRobot and InTouch Health. The machine moves around the hospital to rooms of patients identified by the doctor. Once in a room, it connects the doctor to the patient or hospital staff through the robot’s video screen.
- The buddy system: Researchers at Columbia University found that the pain ratings of hospitalized children dropped significantly when they interacted with “therapeutic robot companions.”
Video bonus: When da Vinci is good, it’s very, very good. Here’s a video of a surgeon using one to peel a grape.
Video bonus bonus: Okay, admittedly this has nothing to do with robotic surgery, but it’s the hottest robot video on the Web right now–an impressive, yet somewhat creepy demo of Boston Dynamics’ “Petman” in camo gear.
More from Smithsonian.com
Gamers Are Better at Robotic Surgery Than Med Students
/https://tf-cmsv2-smithsonianmag-media.s3.amazonaws.com/accounts/headshot/randy-rieland-240.png)